May 2, 2025
Most of us are familiar with an ICRA Permit, the standard one-page generic form that is recycled time and again, from facility to facility. The form, that is (usually) completed by an Infection Preventionist or Hospital Safety Resource just days (or moments) before the project begins. How many times have you performed a project in a hospital and never even seen the documented ICRA plan?
The Infection Control Risk Assessment (ICRA) is a creation and requirement of the Joint Commission’s Accreditation Process for hospitals. If there is a project, there has to be an ICRA or at least a documented determination that an ICRA was not warranted. Technically speaking, “during the programming phase of a construction project, the owner shall provide an Infection Control Risk Assessment (ICRA).”
Hypothetically, let’s say you did receive an ICRA plan document from the Owner with the RFP or even during Pre-Con. Aside from confirming the project title, relative work area and some broad dust control requirements; what did that document do for you? Did it help with phasing? Did it help with budgeting? Did it help with identifying operational constraints that will impact the schedule? Did it consider existing building conditions that will affect the scope of work?
One of the biggest issues with the broad concept measures ‘identified’ in an ICRA plan, is the absence of a clearly identified path to compliance for the workers in the field. In other words, those generic ICRA forms are too broad and do not offer enough guidance to workers in the field. This oftentimes leads to a lot of subjective evaluation that ultimately drives the tradesmen to throw up their hands and view ICRA concepts as an impediment to scope execution.
Here are some of the elements that we feel are imperative in a true infection prevention risk assessment which lead to the necessary clarity, liability protection and ultimately support project success.
Figure 1. Sample Project Phase Drawing from a Comprehensive ICRA Plan Document
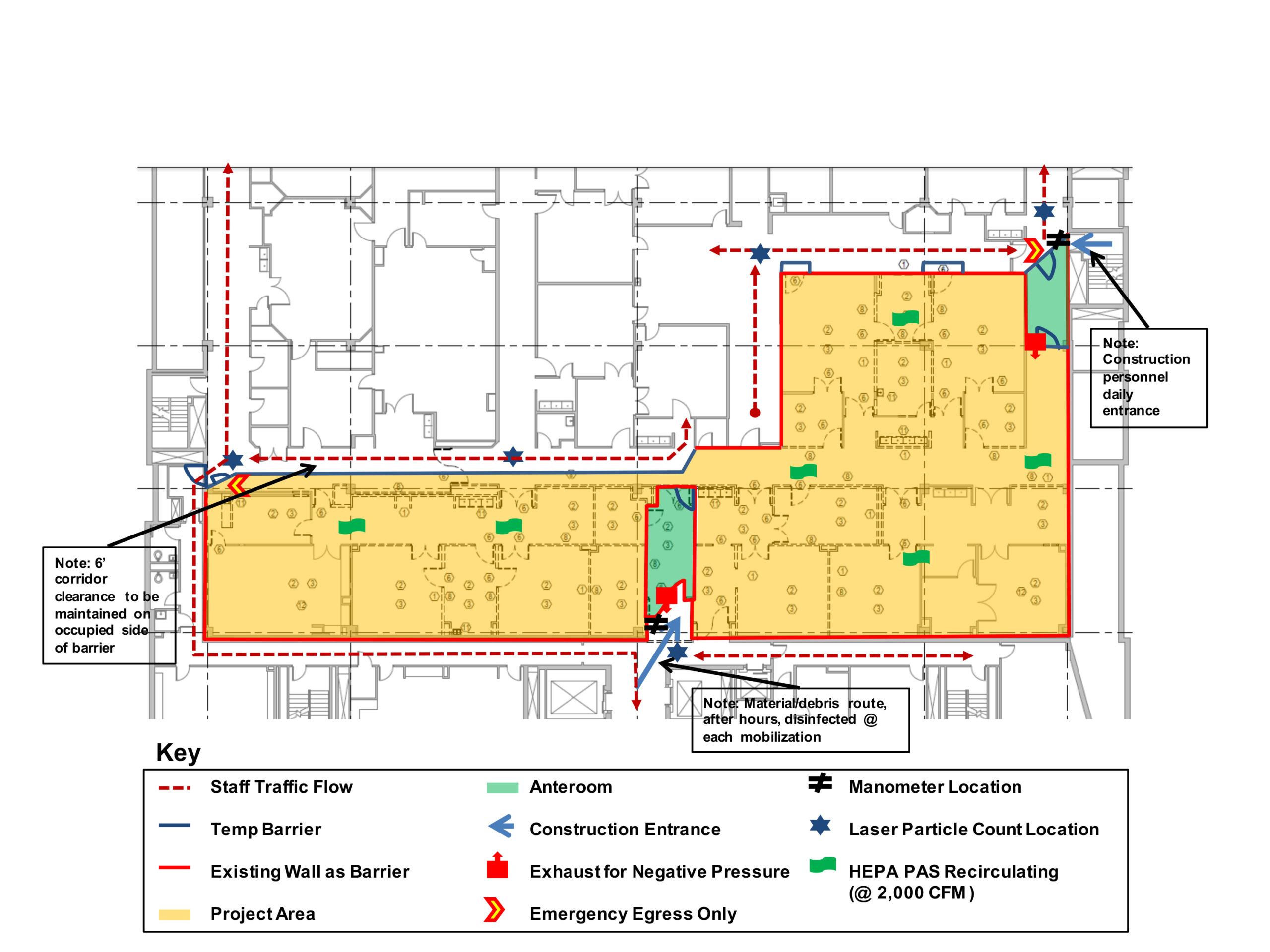
Your comprehensive ICRA plan should include drawings of the hospital work zone and surrounding areas. These drawings should illustrate the Interim Infection Control Protocols that your team has decided on, and include notes of important details. Distribute these drawings to your facility’s infection control team and any contractors who will be working on site.
Narrative on project objectives and constraints:
This may seem a bit obvious, but with the various roles and multitude of individual players’ non-ICRA related project responsibilities the narrative provides an appropriately focused destination description which establishes a framework for route determination.
If we were all headed to Albuquerque from different points of origin, we would need to consider our method of travel, route, durations, potential delays, travel costs, etc. A GPS, travel guide and budget would be extremely helpful in achieving Albuquerque. The narrative lets you know where you’re going, how to get there and alerts you to road blocks you may encounter along the way.
Clear delineation of responsibilities:
How can we expect commitment, compliance and success in the absence of detailing everyone’s role in the mission? There are tasks and components that the General Contractor / Construction Manager must either execute / ensure, if we are to succeed. Additionally, the mission is being conducted in the Owner’s house. There are ground rules and ways that things have historically been done (right and wrong). Before we set off on the mission we want to make sure that key roles are discussed, agreed upon and documented for all hospital staff, contractors and workers in the field.
Subcontractor specific responsibilities:
One of the best insurance policies for proper ICRA implementation is to define what each subcontractor will provide and what their people will do to facilitate project Infection Prevention. This most appropriately goes into their bid packages. That way they can clearly understand expectations on the front end, price things accordingly and be in a position to satisfy the objectives.
Pre-construction testing and documentation:
Your team may be perfectly capable of building a square peg, but the more we know about the round hole it must fit in, the better off we will be. What if the Air Handling Units (AHUs) are currently underperforming or have substantial fungal growth? Maybe we should take a look at the existing caulk joints and window gaskets. Are their trash rooms negative and clean storage rooms positive? Do we anticipate our schedule being held hostage while abatement activities occur? Shouldn’t we?
Think of it this way: Your doctor can’t properly diagnose and prescribe treatment without learning your pre-existing conditions and allergies first, right? If you’re going to prescribe a proper ICRA plan, you should have a hold on what’s going on with the space before you start working.
Specific detail on materials and equipment:
This element directly feeds into effective budgeting which enables the right stuff at sufficient quantities. It’s not a question of how many air machines, it’s a question of how much total airflow we need to budget. Do we need real-time Bluetooth enabled pressure monitors or will analog magnahelics suffice? Will this shop vac be sufficient or do we really need a true HEPA vac? What about bunny suits and shoe covers? Will all tools and equipment need to be disinfected prior to mobilization? How much time will set up cost us? Time is money.
Cleaning methods defined:
There is no more cost effective disinfectant than bleach/water solutions, but that may not work given the surfaces that require continual cleaning. So, what surfaces do we need to clean? What are the best methods and products for disinfection? Will lesser-trained laborers functionally achieve the level of cleanliness needed for the given scope in a given risk area? This should be figured out before you get started.

Barrier locations and composition:
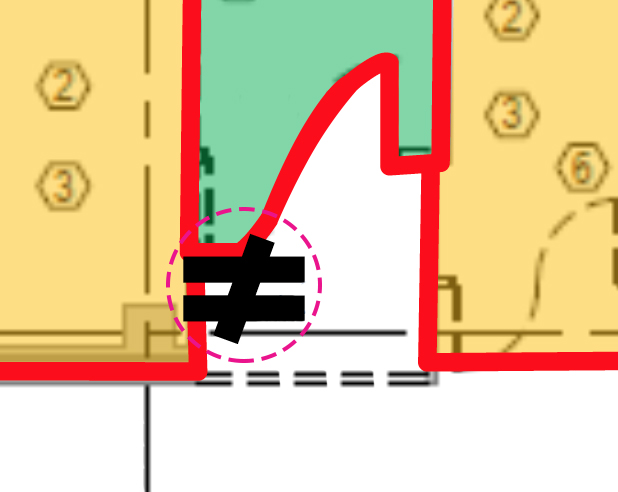
All temporary barriers must be (relatively) airtight and have a cleanable surface. How does phasing impact short term and long term barriers? Even if the barriers were shown by the Architect, will they functionally work, as shown, given operational constraints? Did we consider bed swing radius, egress, pneumatic tube stations, etc. in light of barrier placement?
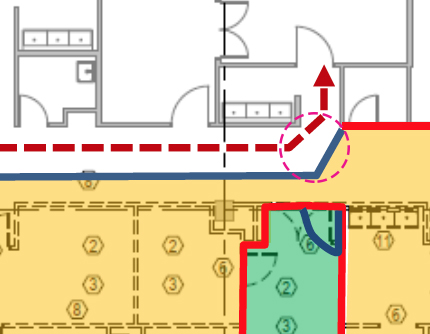
Ensure that temporary barriers are set up to allow for proper traffic flow necessary for daily operations. In this case, temporary barriers had to be set up at an angle to allow enough swing radius for hospital equipment to turn the corner.
![]()
Hospital staff traffic flow around construction:
The Owner staff may not realize how much of an impediment your barriers will be to functional healthcare delivery, until you have already erected them. We must understand their functional needs (and wants) so that our strategy can also facilitate our scope.
 Negative air exhaust route:
Negative air exhaust route:
Stated above, but how much cubic feet per minute (cfm) do we need to exhaust? Do we need the mechanical sub to fabricate a custom transition so we can fit four ducts into one at a window location? Do we need a gooseneck on the roof? If we cannot exhaust to the exterior, what is the best option? By the way, NEVER, EVER exhaust into the returns, regardless of how filtered your air is.
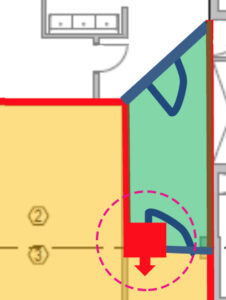
Negative Air Exhaust into work area provides negative pressure in anteroom; additional exhaust is needed for the renovation area.
 Emergency egress routing:
Emergency egress routing:
This would apply to a secondary exit for occupants and in some cases, a safe path for the construction work force. We may need to facilitate rapid bed movement through our phase to an adjacent smoke compartment. How well will that work with ladders, material and job boxes strewn as an array of obstacles?
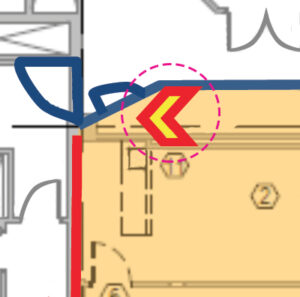
Egress requirements along with other Life Safety Code components should be addressed in the ICRA.
 Construction access/debris routes:
Construction access/debris routes:
With respect to operational needs and higher risk settings, what is the most efficient route to feed the job? How can we reduce the tracking of dust, dirt and debris through patient areas? Is this phase near a service elevator? Do we really think all of our workers will climb five sets of stairs every day, when no one is looking? Shame on us. We want to figure out what should happen, and then enable that should.
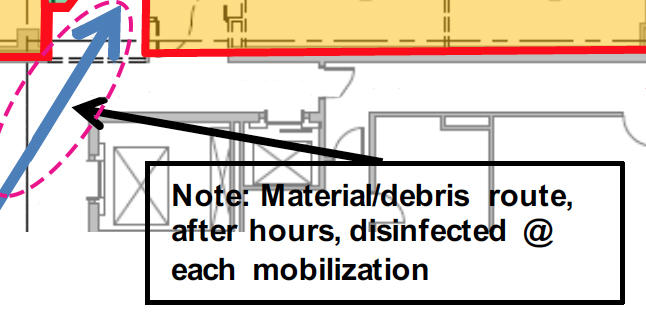
Construction routes should be planned to minimize travel through patient areas. In this case, ideal times for transport and cleaning have also been noted.
 Manometer use / locations:
Manometer use / locations:
We definitely want to know that we are sufficiently negatively pressurized, and also know that we are not too negative. If we become too negative, we can have impacts on perimeter air balance. We would not want our manometer (and corresponding documentation) to go haywire every time the elevator doors open or when two particular sets of doors are simultaneously opened or closed causing air to rush by from smoke compartment to smoke compartment.
Manometers were set up outside this anteroom and near construction access route to ensure that the proper balance of negative pressure was being maintained.
 Particulate monitoring locations:
Particulate monitoring locations:
The primary objective is to control our project-related dust. An ICRA plan is not about how much you $pend, it is about being effective. There is no better way to KNOW that we achieved this objective than by consistently monitoring and documenting airborne dust levels around our project with respect to concurrent outdoor conditions.

Particulate monitoring should be used at work area entrances to ensure anterooms and temporary barriers are effectively containing dust. In this case, a particulate monitoring location has also been set up outside of a long stretch of temporary barriers that is being used to separate hospital traffic flow from the project work area.
Documentation of ICRA QA/QC monitoring:
If it is not in writing, it never happened. All that effort, all of that time and money. We need to make sure that the documentation that we collect proves that patient protection was maintained and that the collected data does not become ammunition for false allegation.
Commissioning and project completion:
Are we or our client relying on “It looks clean” as our acceptance level to permit occupancy by high risk patients? Subjective assessment like this has led to some very costly last-minute measures to address both real and oddly perceived risks. We may want to document air quality inside your new supply air ducts. We might want to discuss methods to demonstrate relative surface cleanliness. We’ve come this far; let’s not throw it all away at the end.
Drawings to support ICRA components:
If you’ve made it to this point in the article, we have some specs you might enjoy reading. But for most folks on the team, a drawing would be easier to digest. The people in the field are comfortable with drawings. All the detail they need is right there. These ICRA plan drawings can be posted at our construction entrances so that even the latest tradesmen to join the project are crystal clear on the requirements AND, we can demand/expect compliance. If we do not effectively communicate with the field who is ultimately responsible for non-compliance?
AMI is here to support you:
We have had the opportunity to help literally hundreds of project teams accomplish their scope of work while effectively satisfying Infection Prevention objectives. ICRA doesn’t have to get in the way. ICRA doesn’t have to be a nightmare. We don’t always have to exhaust our wallets out the window. In fact, some dedicated ICRA planning should make things a whole lot easier. AMI is here to help you protect patients, satisfy your clients, protect your liability and outcompete your competition. For more information on how we can achieve this together please contact AMI Environmental.